ICH GCP Renovation. The way forward

ICH E8 and E6 need modernizing to prepare for the future, a future that will bring future medicines, future trial designs and future data sources [1]. This is the so called ICH GCP Renovation project.
On the 12th of January 2017, following the adoption of the integrated addendum update to GCP, The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) announced their plans for a more extensive revision of ICH-GCP in a reflection paper known as the “GCP Renovation” [2].
The main goals are to provide updated guidance which is flexible enough to address the increasing diversity of clinical trials designs and data sources employed to support regulatory decisions. Also a guidance that is focused on the issues that are more critical for trial quality and that allows the involvement of external stakeholders.
The underlying principles of human subject protection and data quality will remain [2].
Revision Process
First Step: Renovation of ICH E8 General Considerations for Clinical Trials
ICH E8 was finalized in 1997 and has not been updated subsequently. ICH E8 (R1) draft was released for public consultation in May 2019 [3].
The revision proposal focuses on data quality, including the concept of quality by design (QbD) as a key consideration in the study planning phases, which implies designing quality into the study protocol, procedures and associated operational plans.
Quality of a clinical study is considered in this draft document as “fitness for purpose”.
ICH E8 (R1) will include the need to identify a specific set of factors critical to the quality of a given study (critical to quality “CtQ” factors), and the strategies and actions (management of risks) that could effectively support quality in these critical areas to generate reliable data and ensure patients safety [2].
The periodic review of CtQ factors will also be a must since unanticipated issues may appear after the study begins. The review output will determine whether the current risk controls need to be adjusted.
Examples of CtQ factors include [4][5]:
-
Protocol Design
-
Eligibility criteria
-
Randomization
-
Masking
-
Endpoints
-
-
Feasibility and study procedures
-
Patient Safety
-
Informed Consent
-
Withdrawal criteria
-
Data monitoring Committee/ Stopping rules
-
-
Study Conduct
-
Investigator/site qualification
-
Data recording and reporting
-
Statistical analysis
-
-
Study Reporting
-
Communication of results
-
Other important aspect that will be covered is the engagement of multiple stakeholders in the study design, including patients and treating physicians.
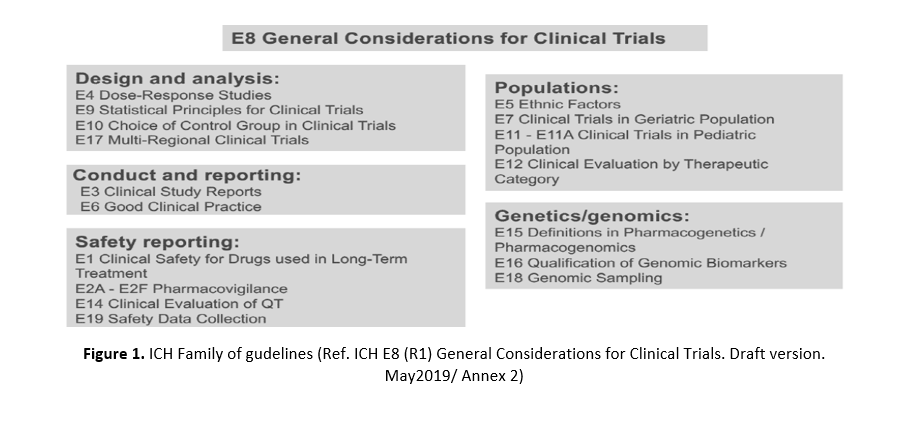
ICH E8 (R1) will also update the cross-referencing to the ICH guidance documents to facilitate study planning [1]. ICH E8 needs to be considered as the cornerstone, the foundation to talk about clinical trials. The ICH E family of guidelines need to be read together (Figure 1).
 Quality should rely on good design rather than on retrospective document checking. Even if monitoring, audits and inspections are key processes, they are not enough to ensure the quality of a clinical trial. The deficiencies identified during these activities imply retrospective corrective and preventative actions, which sometimes include protocol amendments.
Quality should rely on good design rather than on retrospective document checking. Even if monitoring, audits and inspections are key processes, they are not enough to ensure the quality of a clinical trial. The deficiencies identified during these activities imply retrospective corrective and preventative actions, which sometimes include protocol amendments.
It is important to avoid protocol amendments [1], as more complex trials have on average three protocol amendments.
In summary, the key design principles will remain the same: the goal is to obtain high-quality evidence to inform decision-making [4].
Second Step: Renovation of ICH E6 Guideline for Good Clinical Practice
ICH E6 R2 addendum was finalized in 2016. Since it was an addendum, the existing text could not be changed. It is considered as a quick fix that needs to be reoriented.
ICH proposes a subsequent renovation of the current ICH E6 guideline. It will not be an addendum but a full rewrite.
The renovation will preserve a key role for the current focus on traditional interventional trials conducted in a clinical trial setting, while also addressing a broader range of study types and data sources [4].
A relevant addition to the current ICH E6 (R2), will be a set of annexes that will address in more detail the particular study types and/ or data sources:
-
Annex 1: Traditional interventional trials of unapproved or approved drugs.
-
Annex 2: Non-Traditional Interventional Trials or data sources (pragmatic, decentralized clinical trials).
-
Annex 3: Non-Traditional Trial Designs (observational studies, patients registries).
It also plans to provide a more detailed workup of the CtQ factors that should be considered.
This new approach will provide flexibility to ensure the principles remain the same regardless of the study’s objectives or setting.
Timelines and next steps
ICH E8 (R1)
The last public stakeholder workshop focused on ICH E8 (R1) was held on the 31st of October 2019 in Washington DC (USA) [4].
Two Experts Working Group (EWG) face to face meetings are expected in March and May 2020.
Finalization of the guidance document is expected in June 2020 [4].
ICH E6 (R3)
The first face to face meeting to produce the ICH concept paper is planned for the 15-18th of November 2019 in Singapore. Work on the overarching principles and Annex 1 will continue.
The overall estimated timeline for the adoption (step 4) of E6 is mid-2021. The adoption of E6 Annex 1 is estimated by the end of 2022, early 2023 [1].
Conclusion
The key message of the GCP Renovation project is that this venture is about changing the way we do things.
We need to readjust the way we approach clinical trials since the clinical research arena is evolving and the current guidance will not be appropriate any longer, as data sources and other factors are expanding.
Fit-for-purpose clinical trials need to be promoted by achieving quality by good design. But how can we do that?
By introducing the quality by design concept and identifying critical to quality factors. In simple words, think first about the design, those aspects that are critical for the specific study and then do the work.
The quality of the information and the reliability of the data generated should be enough to support good decision making.
Consider all parties, including patients and treatment physicians, when setting the foundations for the study design.
References
-
Sweeney. GCP Renovation – ICH E8 and ICH E6. 3rd European QA Conference, Dublin. November 2019
-
ICH Reflection on “GCP Renovation”: Modernization of ICH E8 and Subsequent Renovation of ICH E6. January 2017
-
ICH E8 (R1) General Considerations for Clinical Trials. Draft version. May2019
-
ICH Public Meeting E8 (R1) General Considerations for Clinical Studies. October 2019
-
CTTI-Clinical Trials Transformation Initiative. Exploring the critical to quality (CTQ) factors (https://www.ctti-clinicaltrials.org/toolkit/qbd/introduce-qbd/qbd-principles/explore-ctq-factors)


